|
|
|
| Endodontic Management Of Bilateral Taurodontism In Impacted Permanent Molars: A Rare Case Report |
Suraj Arora 1 , Tarun Kumar 2 , Priyanka Saluja 3 , Rakesh Singla 4
1 Reader, Dept. of Conservative Dentistry - J.C.D Dental College Sirsa, Haryana
2 Senior Lecturer, Dept. of Conservative Dentistry - J.C.D Dental College Sirsa, Haryana
3 Lecturer, Dept. of Conservative Dentistry - J.C.D Dental College, Vidyapeeth Sirsa, Haryana
4 Reader, Dept. of Conservative Dentistry - J.C.D Dental College, Vidyapeeth Sirsa, Haryana
|
| Address For Correspondence |
Dr. Suraj Arora,
Reader: J.C.D Dental College, Vidyapeeth Sirsa
Email : surajarorasgrd@yahoo.co.in
Ph : 9468319703, 9041828632 |
| Abstract |
| Taurodontism can be defined as a change in tooth shape caused by the failure of Hertwig’s epithelial sheath diaphragm to invaginate at the proper horizontal level. An enlarged pulp chamber, apical displacement of the pulpal floor, and no constriction at the level of the cemento-enamel junction are the characteristic features. Although permanent molar teeth are most commonly affected, this change can also be seen in both the permanent and deciduous dentition, unilaterally or bilaterally, and in any combination of teeth or quadrants. Despite the clinical challenges, taurodontism has received little attention from clinicians. This case report presents a case of a twenty seven year old male patient presented with taurodontism involving the molars of two quadrants, which was not associated with any other anomalies or syndromes. |
|
| Keywords |
| dens in dente, dens invaginatus, pulp necrosis, periapical pathology, MTA retroseal. |
|
| Full Text |
Introduction:
Taurodontism is a developmental disturbance of a tooth that lacks constriction at the level of the cementoenamel junction (CEJ). It is characterized by vertically elongated pulp chamber, apical displacement of the pulpal floor and bifurcation or trifurcations of the roots.[1] The term “taurodontism” (‘bull tooth’) was coined from the Latin word “tauros”, which means ‘bull’ and the Greek word “odus”, which means ‘tooth’. Sir Arthur Keith in 1913 coined the term “taurodontism” and defined taurodontism as “a tendency for the body of the tooth to enlarge at the expense of the roots”.
Shaw (1928) further classified taurodont teeth according to their severity into hypo-, meso- and hypertaurodont forms, hypotaurodontism being the least pronounced form, mesotaurodontism the moderate form and hypertaurodontism
being the most severe form in which the bifurcation or trifurcation occurs near the root apices[2] ( Fig 1).
 | Fig 1.Diagrammatic representation of a) normal (cynodontic) tooth b) hypotaurodont c) mesotaurodont d) hypertaurodont
 |
Later in 1978 Shiffman and Chanannel established mathematical criteria which areadopted by various authors for assessing their cases. According to this criteria, a tooth is considered as a taurodont if the distance from the lowest point of roof of the pulp chamber (A) to the highest point of the floor (B), divided by the distance from A to the root apex (C) is equal to or greater than 0.2 mm, and when the distance from B to the CEJ (D) is greater than 2.5mm (Fig 2). The etiology of taurodontism is unclear. The possible causes of taurodontism have been enumerated by Mangion[3] as follows: 1) A specialized or retrograde character, 2) A primitive pattern, 3) AMendelian recessive trait,4) An atavistic feature, and 5) A mutation resulting from odontoblastic deficiency during dentinogenesis of the roots.
 | Fig 2. Diagram showing Shiffman and Chanannel’s criteria for diagnosing Taurodontism.
|
According to Hamner et al., taurodontism is caused by the failure of Hertwig’s epithelial sheath diaphragm to invaginate at the proper horizontal level.[4] In addition, it has been reported that many patients with the Klinefelter syndrome exhibit taurodontism, but it is not a constant feature of this syndrome. Today, it is considered as an anatomic variant that could occur in a normal population. The prevalence of taurodontism is reported to range from 2.5% to 11.3% of the human population. This range is accounted for by variations in race and differences in diagnostic criteria.
Case Report:
A twenty seven year old male child was brought to dental clinic, sirsa with complain of pain related to left and right posterior tooth region of mandible for last two weeks. There was no significant dental or medical complaint in the past. His intraoral examination revealed normal soft tissue appearance with a large carious lesion in impacted mandibular left and right third molar and patient was not willing for extraction. At the time of examination, the teeth were tender on percussion.
Intraoral periapical radiograph of both sides revealed large pulp chambers and short roots. There were periapical lesions involving both the teeth (Fig 3).
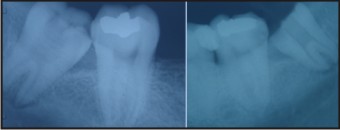 | Fig. 3 Preoperative radiograph of mandibular right and left third molar teeth
|
No other remarkable dental findings were observed clinically or radiographically. Past medical history was non contributory. General physical examination did not reveal any significant findings. Patient’s physical and mental development was with in normal rates for his age.
Based on clinical and radiographic findings, a diagnosis of chronic apical periodontitis was made in relation to mandibular left and right third molar teeth. The right molar was mesotaurodant and the left was hypotaurodont. The right molar was first anaesthetized, the access was opened under isolation and the access cavity was modified. The remaining pulp tissue was extirpated. The pulp was voluminous, to ensure complete removal, 2.5% sodium hypochlorite was initially used as an irrigant to soften the pulp.
Once the pulp was extirpated, further irrigation was done with normal saline. The pulp chamber was huge and the floor of the chamber could not be visualized. At the furcation area, three canal orifices were found: mesiobuccal, mesiolingual, distal. A working length radiograph was taken with #15 file in all the canals and biomechanical preparation was done with Protaper system.
After completion of instrumentation, a calcium hydroxide dressing was given for two weeks. A modified obturation technique was used because of the proximity of the orifices. After drying the canals, AH plus
(Dentsply International) sealer was applied onto the root canal walls with a lentulospiral. The premeasured master cone was coated with sealer and slowly moved to full working length.
Thus, all the canals were obturated. After that, the elongated pulp chamber was obturated with vertical compaction of warm gutta percha.Similarly treatment was done for the left side mandibular molar. Both the obturations could be seen in the radiographs.(Fig 4)
 | Fig 4. Post operative radiograph
|
Discussion
A taurodont tooth shows wide variation in the size of the pulp chamber, varying degrees of obliteration and canal configuration, apically positioned canal orifices. Endodontic treatment in taurodontism teeth has been described as a complex and difficult procedure. Pulp therapy for taurodonts is a challenging treatment, with increased incidence of haemorrhage during access opening which may be mistaken for perforation. Since the roots are short and pulpal floor is placed apically, care should be taken to prevent perforation.[1],[5]
Taurodontism is a dental anomaly characterized by large pulp chambers and short roots. Roots often bifurcate or trifurcate at a low level. They are thought to result from failure of the Hertwig’s epithelial root sheath to invaginate at the proper time. The most frequently affected teeth are the molars. The distance between the baseline connecting the two CEJ and the highest point in the floor of the pulp chamber are used in determining taurodont teeth. Taurodontism is diagnosed in molars when this distance exceeds 2.5 mm.[6]
Taurodontism is associated with several developmental syndromes and anomalies including amelogenesis imperfecta, Down’s syndrome, ectodermal disturbance, Klinefelter syndrome, tricho-dento-osseous syndrome, Mohr syndrome, Wolf-Hirschhorn syndrome and Lowe syndrome.’[7]
From an endodontist’s view, taurodontism presents a challenge during negotiation, instrumentation and obturation in root canal therapy.
Conclusion:
It is very important for a general dental practitioner to be familiar with taurodontism not only with regards to clinical complications but also its management. Taurodontism also provides a valuable clue in detecting its association with many syndromes and other systemic conditions.
References
1. Jafarzadeh H, Azarpazhooh A, Mayhall JT (2008). Taurodontism: a review of the condition and endodontic treatment challenges. Int Endod J 41, 375-38.
2. Shaw JC (1928) Taurodont teeth in South African races. J Anat 62, 476-498.
3. Mangion JJ (1962) Two cases of taurodontism in modern human jaws. Br Dent J 113, 309-312.
4. Hamner JE III, Witkop CJ Jr, Metro PS (1964) Taurodontism: report of a case. Oral Surg Oral Med Oral Pathol 18, 409-418.
5. Rao A, Arathi R (2006) Taurodontism of deciduous and permanent molars: report of two cases. J Indian Soc Pedod Prev Dent 24, 42-44.
6. Shifman A, Chanannel I (1978) Prevalence of taurodontism found in radiographic dental examination of 1,200 young adult Israeli patients. Community Dent Oral Epidemiol 6, 200-203.
7. Joseph M (2008) Endodontic treatment in three taurodontic teeth associated with 48, XXXY Klinefilter syndrome: a review and case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 105, 670-677. |
|
|
|
|
|
|